d o t o r e g . c o m
t o r e g . c o m
Dr. Mete ALPASLAN
Tall R Wave in Lead V1 (C1)
Causes
 Right bundle branch block (most common).
Right bundle branch block (most common).
Right ventricular hypertrophy
Posterior myocardial infarction
Wolff-Parkinson-White (WPW) syndrome
Dextrocardia
Hypertrophic cardiomyopathy
Misplacement of chest electrodes
Normal variant
Reference
Am J Emergency Medicine 2001;19:504-513.

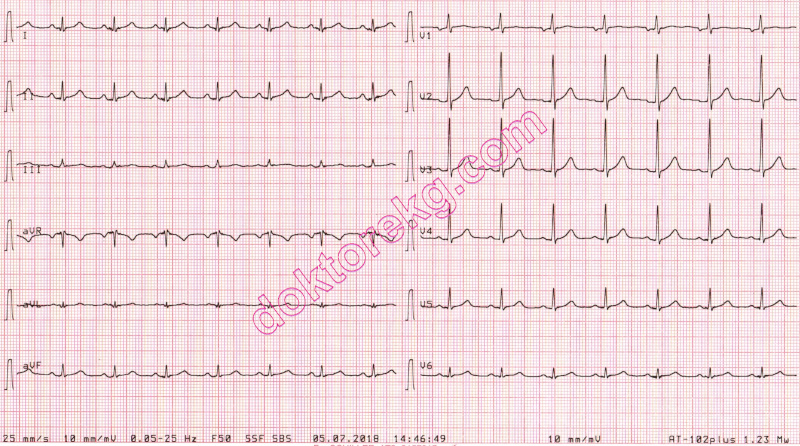
ECG 1. The compact ECG above is from a 51 years-old man. Two years ago, he had experienced acute posterior myocardial
infarction due to total occlusion of the dominant Circumflex (Cx) coronary artery.
The R wave in leads V1 and V2 are taller (and wider) than expected.

ECG 2a. The ECG above belongs to a 46 years-old man with mild mitral stenosis and frequent attacks of palpitation.
At first glance, the q waves in inferior leads and tall R waves in lead V1 suggest a diagnosis of old inferoposterior
myocardial infarction. The delta waves in some patients with WPW syndrome may imitate q waves suggesting old myocardial
infarction.
In the above ECG, lead V3 shows a giant delta wave, while leads V4 and aVL show subtle delta waves.
Click here for a more detailed ECG

ECG 2b. The above ECG was recorded during one of his palpitation attacks.
During the tachycardia, AV-node, His bundle and Purkinje fibers are used for conduction to the ventricles
and the accessory pathway is used for re-exciting the atria: orthodromic AVRT (AV Reciprocating Tachycardia).
Because of this, delta wave is not seen during the tachycardia.
Because of this, tall R wave in lead V1 is not seen during the tachycardia.
Because of this, the ECG above looks very similar to the post-ablation resting ECG below (ECG 9c).
Click here for a more detailed ECG

ECG 2c. Electrophysiologic study showed left posterolateral accessory pathway in this patient.
The above ECG was recorded after ablation of the accessory pathway.
Inferior leads do not show q waves anymore. No more suggestion of old inferoposterior myocardial infarction.
Lead V3, V4 and aVL also do not show delta waves any more.
Click here for a more detailed ECG
ECG 3a. The ECG above, belongs to a 49 years-old man who had experienced acute (now OLD) posterior wall myocardial
infarction several years ago.
The infarction was due to occlusion of the Circumflex (Cx) coronary artery. His right coronary artery was normal.
ECHOcardiography on the same day showed dyskinesia of the left ventricular posterior wall.
This ECG shows tall R waves in leads V1 to V3 which should raise the suspicion of old posterior wall myocardial infarction.
Click here for a more detailed ECG

ECG 3b. The ECG above belongs to the same patient.
However, this time leads V7, V8 and V9 were recorded to show the posterior left ventricular wall directly.
The leads V7 to V9 show q waves but no ST segment elevation (old posterior wall myocardial infarction).
Click here for a more detailed ECG
Right bundle branch block (most common).
Right ventricular hypertrophy
Posterior myocardial infarction
Wolff-Parkinson-White (WPW) syndrome
Dextrocardia
Hypertrophic cardiomyopathy
Misplacement of chest electrodes
Normal variant
Reference
Am J Emergency Medicine 2001;19:504-513.
ECG 1. The compact ECG above is from a 51 years-old man. Two years ago, he had experienced acute posterior myocardial
infarction due to total occlusion of the dominant Circumflex (Cx) coronary artery.
The R wave in leads V1 and V2 are taller (and wider) than expected.
ECG 2a. The ECG above belongs to a 46 years-old man with mild mitral stenosis and frequent attacks of palpitation.
At first glance, the q waves in inferior leads and tall R waves in lead V1 suggest a diagnosis of old inferoposterior
myocardial infarction. The delta waves in some patients with WPW syndrome may imitate q waves suggesting old myocardial
infarction.
In the above ECG, lead V3 shows a giant delta wave, while leads V4 and aVL show subtle delta waves.
Click here for a more detailed ECG
ECG 2b. The above ECG was recorded during one of his palpitation attacks.
During the tachycardia, AV-node, His bundle and Purkinje fibers are used for conduction to the ventricles
and the accessory pathway is used for re-exciting the atria: orthodromic AVRT (AV Reciprocating Tachycardia).
Because of this, delta wave is not seen during the tachycardia.
Because of this, tall R wave in lead V1 is not seen during the tachycardia.
Because of this, the ECG above looks very similar to the post-ablation resting ECG below (ECG 9c).
Click here for a more detailed ECG
ECG 2c. Electrophysiologic study showed left posterolateral accessory pathway in this patient.
The above ECG was recorded after ablation of the accessory pathway.
Inferior leads do not show q waves anymore. No more suggestion of old inferoposterior myocardial infarction.
Lead V3, V4 and aVL also do not show delta waves any more.
Click here for a more detailed ECG
ECG 3a. The ECG above, belongs to a 49 years-old man who had experienced acute (now OLD) posterior wall myocardial
infarction several years ago.
The infarction was due to occlusion of the Circumflex (Cx) coronary artery. His right coronary artery was normal.
ECHOcardiography on the same day showed dyskinesia of the left ventricular posterior wall.
This ECG shows tall R waves in leads V1 to V3 which should raise the suspicion of old posterior wall myocardial infarction.
Click here for a more detailed ECG
ECG 3b. The ECG above belongs to the same patient.
However, this time leads V7, V8 and V9 were recorded to show the posterior left ventricular wall directly.
The leads V7 to V9 show q waves but no ST segment elevation (old posterior wall myocardial infarction).
Click here for a more detailed ECG